204 – Tracheal Stenosis

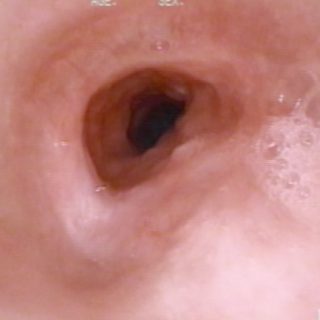
Central and critical tracheal stenosis. Smooth and tense appearance due to congestive edema of the mucosa. Cetrángolo Hospital

Central and critical tracheal stenosis. Smooth and tense appearance due to congestive edema of the mucosa. Cetrángolo Hospital

Double stent: after the endo-surgical resection of an extensive carcinoma, two silicone stent were applied in the tracheal bifurcation, leaving the carina “enclosed” between them. In the image, the generalized edema dominates the field and very abundant mucopurulent secretions accumulate around the prosthesis and inside one of them, in which a bubble has formed at … Read more
Appearance of the tracheal mucosa after the removal of a stent. There is an arch of residual stenosis, still congestive, and a mucosal bed with bulging edema due to prolonged contact with the prosthesis in that area.

Tracheal Stent after 10 months remain implanted. The walls of the endoprosthesis are free of secretions and incrustations, but several granulomas have developed in the mucosa close to its distal end. One, very bulky and bulgy, sits on the entire back wall.
“Ideal” position for a tracheal stent in the treatment of unresectable stenosis. The device is “trapped” in the area of the stenosis and its anterior end is “floating” in the tracheal lumen. Thus, this position reduces the possibility of the appearance of granulomas. The distal end of the prosthesis is still somewhat folded. The defect … Read more
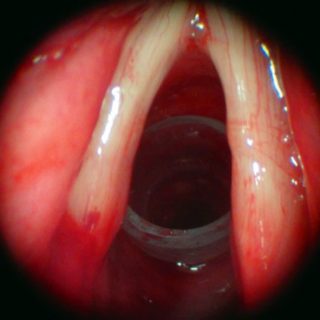
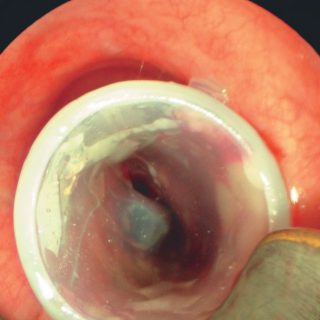
Silicone stent acting as a support in a tracheal stenosis at the level of the first rings. The vocal cords are somewhat thickened and with obvious congestion in the mucosa in its posterior third, close to the arytenoids.

Complex tracheal stenosis after endo-surgical treatment. Image taken one month after a stent, that remained for 2 years, was removed. There is sufficient tracheal light and some changes in its relief due to the presence of granulomas on the left wall. The edema erases the longitudinal folds and the silhouette of the cartilages.
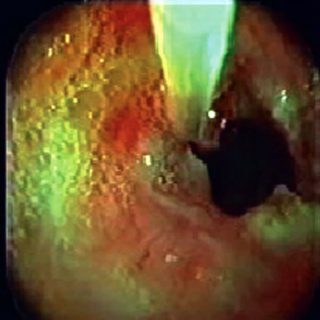
Radial cuts at hours 3 and 9, performed with electrocautery. Procedure prior to dilation of a simple tracheal stenosis. The radial cut is also a safety measure reducing the risks of rupture of the posterior membrane during the dilation maneuvers.

In this tracheal compression, the magnitude is such that there is no light in the right source bronchus and a large reduction in crescent in the left. The “Y” stent is indicated to recover light and threatened ventilation.