259 – Bronchial Carcinoma

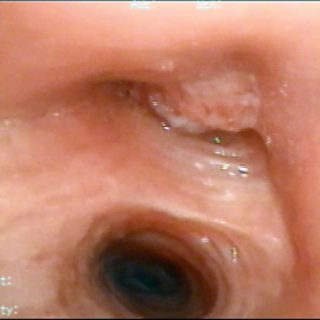
Deformation of the entrance of the lower left lobar bronchus. Its circumferential contour is now wavy. There are changes in vascularization and several submucosal protrusions.

Deformation of the entrance of the lower left lobar bronchus. Its circumferential contour is now wavy. There are changes in vascularization and several submucosal protrusions.

View from the left source bronchus, near its fork in the carrefour. A prominent mass rises on its side and bottom walls. The longitudinal folds, very accentuated, lose their parallelism and tend to meet as they enter the upper and lower lobe bronchi. The widening of the secondary carina and the intense edema contribute to … Read more

Tumor with “glove finger” appearance. This lesion emerges from the right source bronchus and its independence from the bronchial wall is quite evident. It may have a base of implantation much farther from its visible proximal end. The tracheal carina is pushed to the left.

With a rather classic appearance, this large formation with large submucosal vessels, arises from the posterior tracheal wall and also from the angle that it forms with the lateral walls, as usually happens in adenoid cystic tumors.
Location combination: Endoluminal vegetative formation and intramural lesion are present in this subocclusive lesion of the right upper lobe.

Trachea severely affected by a carcinoma that sits on the posterior wall of the intrathoracic and precarinal portion with 50% light reduction.

Inflammatory signs dominate the image, but here the light has been lost and the longitudinal folds meet giving this upper lobe a “funnel” aspect: “Bence sign”. This indirect sign linked to bronchogenic carcinoma was described in Buenos Aires in 1942 by Dr. Alvaro Bence, in charge of the bronchoscopy service at the Guillermo Rawson hospital … Read more

Example of “intramural” injury. The tumor deforms the light by occupying the wall without destroying the mucosa yet. Positive biopsy. Undifferentiated carcinoma.

This carcinoma occurs in the trachea with a very smooth surface which will suspect a carcinoid tumor. Note the intense mucosal vascularization that with a more or less parallel disposition is directed to the tumor.

All signs present: Vegetative tissue, with whitish necrotic areas, mamelons, edema, changes in vascularization and coloration with more or less congestive areas, in this carcinoma that occludes the intermediate bronchus.