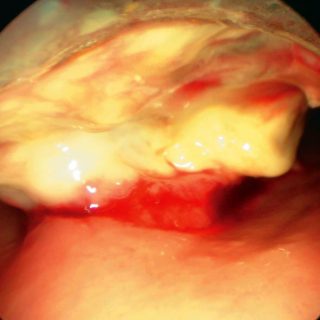
273 – Epidermoid Bronchial Carcinoma
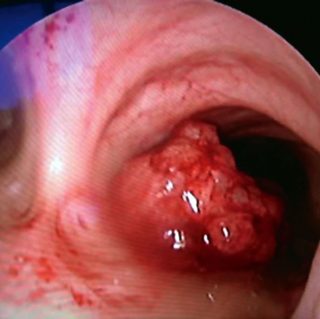
A vegetative formation sits on the right side of the carina. It presents multiple mamelons that give it an irregular and hyperemic aspect that contrasts with the general pallor of the healthy mucosa. An ecchymotic dot is distributed in the area of the edge of the main carina and in its posterior triangle. Squamous cell … Read more