
183 – Blind Trachea
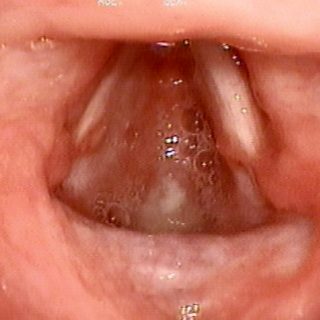
Laryngeal stenosis that has evolved towards the total closure of light at the level of the subglottis. The patient suffers a post-intubation rash with damage to the laryngeal cartilages. It develops a subglottic stenosis that, when it becomes symptomatic or critical, receives the relief of the tracheostomy at the hands of the surgeon. However, this … Read more






