205 – Stents and Stenosis

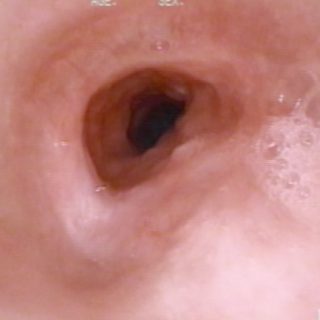
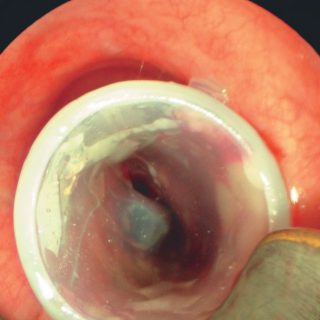
After implanting this “Y” shaped stent, the advance of tumor growth into the stent makes it emerge through its right bronchial branch. As an undesired consequence of the subocclusion of this source bronchus, there is an accumulation of secretions at its entrance, indicating a precarious airflow and an ineffective cough.